live better, longer
If you are working on your bone health, you already know the feeling. You make changes. You train. You take supplements. You fix your diet. You do all the right things, and then you wait.
And you wait.
Because your next DEXA might not be for a year. Sometimes two years. That is a long time to stay motivated when you have no feedback.
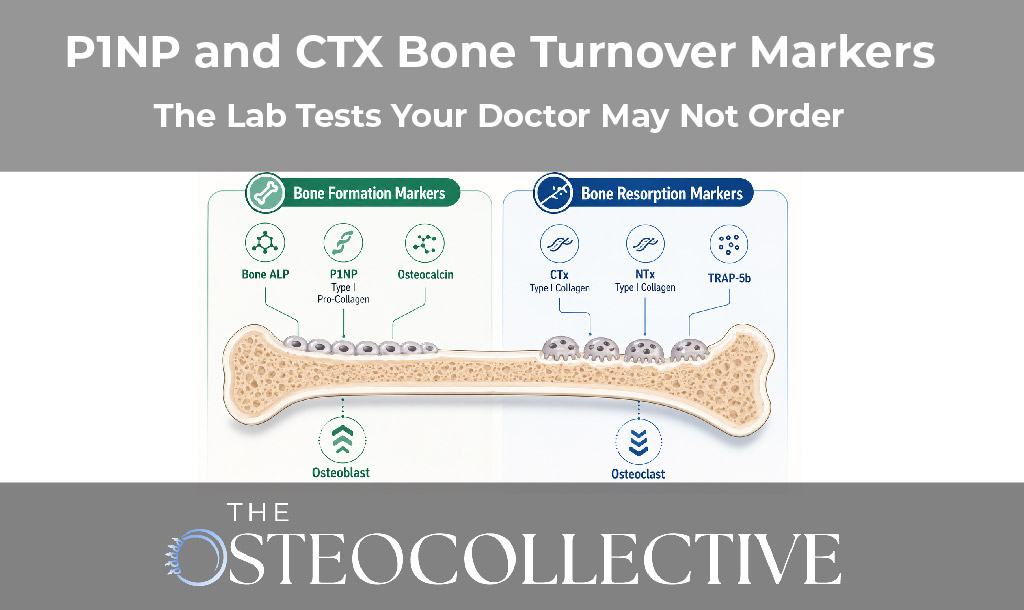
This is why I recommend two lab tests for many patients who are trying to improve bone health. They are bone turnover markers. The two I like most are P1NP and CTX.
These labs do not replace imaging. We still want DEXA or REMS. But these labs can help you see what is happening sooner. They can help you adjust your plan before you waste a year doing the wrong thing.
Let’s keep this simple.
P1NP is a bone building marker. It tells us what the bone building cells, the osteoblasts, are doing.
CTX is a bone breakdown marker. It tells us what the bone breakdown cells, the osteoclasts, are doing.
Bone is not static. Bone is alive. It is always breaking down and building back up. If breakdown is too high, you lose bone. If building is too low, you lose bone. If we want you to improve, we need the balance to move in the right direction.
DEXA is useful. It is the most common scan. It gives us a density score. But it has limitations.
First, DEXA is slow to change. Even in a strong program, you may not see a clear change for 12 to 24 months.
Second, DEXA has a margin of error. Small changes might not be “real” changes. You can improve a few percent and still not feel sure what happened.
REMS can be better in some ways. It adds a quality score. But even REMS is not instant. And not everyone has access to REMS.
So here is the big question.
What can we measure in the short term to see if your plan is working?
That is where bone turnover markers come in.
Bone turnover markers can help you do three things:
These labs are not perfect. But they give us early clues. And early clues help you avoid wasted time.
This is a big frustration. People ask their doctor for CTX and P1NP and get shut down.
Most of the time, it is not because the doctor is evil. It is because of how the system works.
Here are the main reasons.
In a standard clinic model, labs are ordered to change therapy. Many doctors use CTX and P1NP only to monitor drug therapy, not lifestyle therapy.
If you are not taking a bone drug, they may feel there is no reason to order the test.
Many doctors were never trained to use these labs for exercise, nutrition, or hormone plans. So even if they order it, they may not know what to do with it.
Doctors worry about liability. A lab result can lead to a recommendation. A recommendation can lead to risk. Many doctors avoid tests that push them outside their usual protocol.
This is the part most people do not understand until it happens to them.
The cash price for a lab can be very different than the insurance billed price. And if insurance denies it, you may get a large bill.
That risk alone causes many doctors to say no.
Here is the big picture.
Our medical system is built for acute care. It is great at emergencies. It is great at surgery. It is great at drugs.
But osteoporosis is a chronic disease. Preventing it and reversing it often takes:
That is a different model. That is why I often say the “standard system” is not built for this goal.
You can still use your doctor for what they do best. But if you want prevention and optimization, you may need additional support outside that model.
If you want to reverse osteoporosis naturally, you need feedback.
We use bone turnover markers to help answer questions like:
These labs are not a “magic test.” But they let us see the direction of the trend.
There is not one perfect answer.
Here is the simple version:
These labs can shift based on the time of day and food. P1NP in particular can change based on whether you ate.
If you want clean data, you need consistent conditions.
You are trying to measure the trend, not a random swing.
This is where people get stuck. The math looks annoying, but it is not that bad.
P1NP and CTX use different units. So we adjust CTX by dividing it by 1000.
Then we calculate:
P1NP ÷ (CTX ÷ 1000)
Example:
First adjust CTX:
Now divide:
Higher is better. That means you have more building compared to breakdown.
Right now, we often use 150 as a practical threshold.
It is not perfect. It is not a guarantee. But in our experience, people who move this ratio above that range tend to do better over time.
If you are on drugs like bisphosphonates or Prolia, these markers can be very suppressed.
CTX can drop to extremely low levels. P1NP can also drop very low. That can make the ratio look “good” even when bone turnover is too low.
So if you are on drug therapy, you need to interpret these labs differently.
You can ask your doctor. Some will order them. Many will not.
If you do get them through insurance, be aware that coverage can vary. And if denied, the bill can be large.
In our community, we make it easier to access these labs and understand them. We also try to keep costs more predictable, because we want people to be able to track progress without financial surprises.
A lot of people do bone health like this:
That is painfully slow. Bone is slow, yes. But your feedback loop does not have to be that slow.
P1NP and CTX shorten the loop. They give you data sooner. That helps you make better decisions.
If you are unsure what to do next, join my free Bone Health Masterclass. I walk through the biggest mistakes we see and how to build a plan that actually fits your life.
And if you want ongoing support, lab access, community, and deeper guidance, consider joining The OsteoCollective.
This content is for educational purposes only and is not medical advice. Lab tests should be interpreted in the context of your full medical history and medications. Do not start, stop, or change supplements, exercise, or medications based on this content without speaking with your physician or qualified healthcare provider.

Your Blueprint for Lasting Bone Health and Longevity
.svg)
.svg)
.svg)
.svg)
Join us LIVE July 30th, 2026 at 3:00pm EST to Learn Dr. Doug's proven framework for Osteoporosis Reversal for FREE. Yes! Reversing Osteoporosis is possible and has happened for hundreds of Dr. Doug's patients.
If you have been blind-sided, feel stuck, confused, and exhausted with your diagnosis, this Masterclass is for you!

.svg)

.svg)
