live better, longer
What if there was a way to use a bisphosphonate drug like Reclast (zoledronate) as a long-term fracture prevention plan?
That is exactly what a newer study suggests. And at first glance, it sounds like the “easy button” for osteoporosis. One infusion now. Maybe one more in five years. Then a decade of protection.
If that were true for everyone, I could stop talking about protein, strength training, impact work, sleep, hormones, and the whole lifestyle plan.
But the truth is more complicated.
This post breaks down what the study did, what it found, and why the results are real and still not a “drug-only” solution for most people.
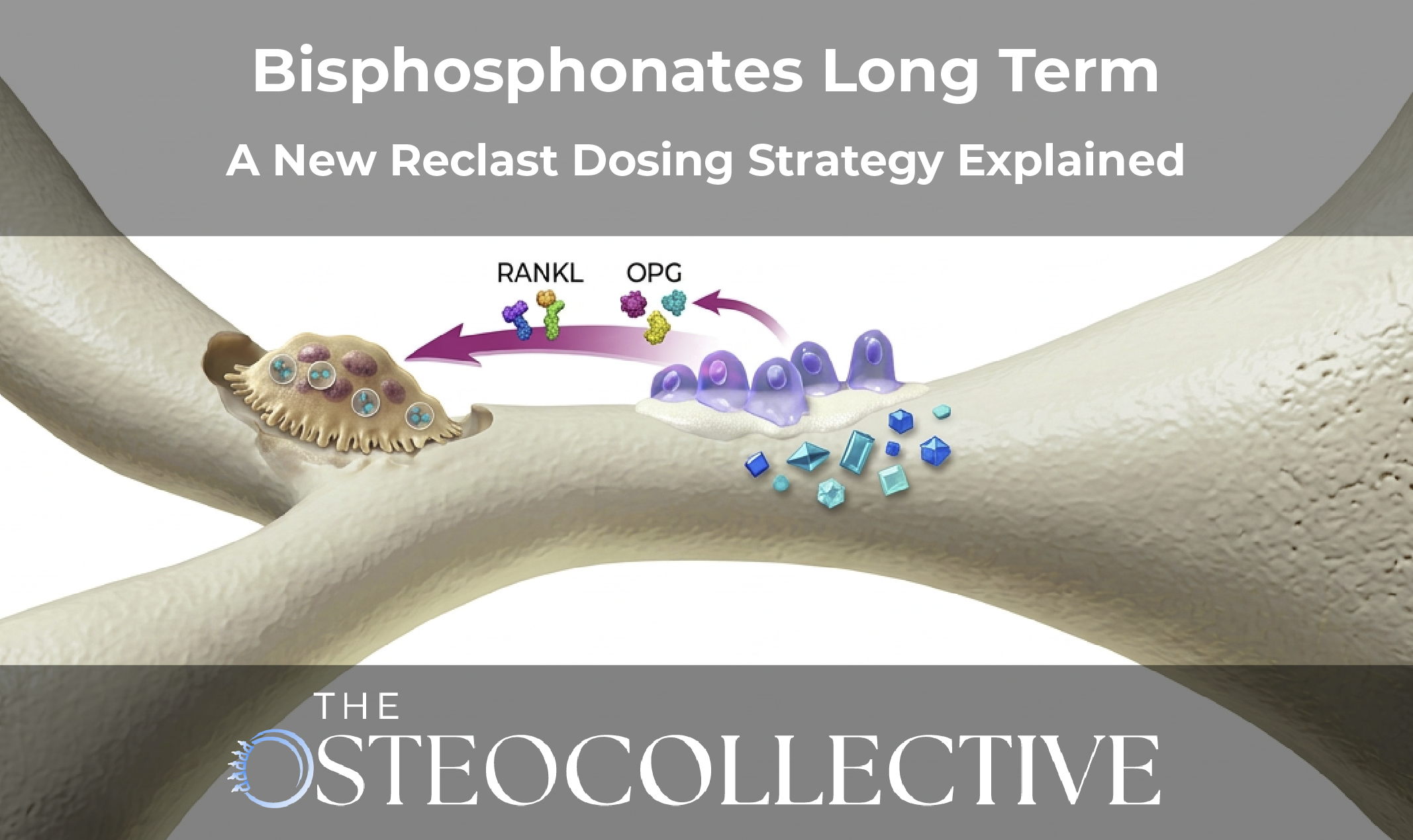
Bisphosphonates are anti-resorptive drugs. That means they slow down bone breakdown.
They do this by binding to bone. When osteoclasts (the bone breakdown cells) try to resorb bone, they take in the drug and get shut down. That leads to lower bone resorption and higher bone density in the short term.
That can be helpful. But there is a tradeoff.
Bone is not supposed to be frozen. Bone is living tissue. It needs turnover and remodeling to stay strong.
If you suppress turnover too hard for too long, you can raise the risk of rare but serious issues, like:
That is part of why guidelines often recommend stopping after 3 years for IV therapy or 3–5 years for oral therapy, followed by a “drug holiday.”
The big problem is that drug holidays are messy. How long should they be? When do you restart? Which drug do you restart? Do you switch to an anabolic? There is not one clean answer.
That is why a study about long-term infrequent dosing is so interesting.
This trial was published in the New England Journal of Medicine and included a little over 1,000 women.
The age group was important:
And also this key point:
So these women did not have osteoporosis at baseline. Some had low bone density, but they were not in the osteoporosis range.
The study used zoledronate (Reclast) 5 mg:
Then they followed the women for 10 years.
They did several useful things:
That last part matters. I love when studies include turnover markers, because it shows what is happening under the hood.
Over 10 years:
So the two-dose approach did reduce vertebral fracture outcomes over 10 years.
That is a real outcome. And it is statistically meaningful.
If you are in a group that truly needs this approach, that is a win.
But we also need to be honest about what “vertebral fracture” means in these trials.
Morphometric fractures are found by x-ray measurement. It means a vertebra looks compressed on imaging.
Some of these fractures are painful and obvious. Some are silent. They are still relevant. But they are not the same as a hip fracture that sends someone to the hospital.
So yes, a reduction here matters. But it is still not the entire story.
Now let’s talk DEXA.
This was the pattern:
That is not surprising. Bisphosphonates usually show stronger effects in trabecular-rich bone (spine) than cortical-heavy bone (hip).
In the placebo group, by year 10, lumbar spine bone density dropped about 6%.
That is what you expect in this age group when you exclude hormone therapy and other strong bone tools.
This is where it gets interesting.
The one-dose group increased early, then started to decline over time.
The two-dose group increased early and held better, but it did not keep climbing forever.
In the hip, even the two-dose group drifted back toward baseline by year 10.
So what does that tell us?
It suggests there may be a ceiling effect. The drug helps, but it does not keep stacking gains forever.
This is the part that matters most to me.
They measured:
And yes, you see what you expect:
That second point is the one many people miss.
If you suppress breakdown, you often suppress building too.
Even at 10 years, after a single infusion, bone turnover markers were still suppressed.
Not massively suppressed, but still below baseline.
This tells you how long this drug can stay active in the body.
That matters for consent. If you do not want long-term suppression, you need to know what you are signing up for.
This also explains why “drug holidays” are so confusing. The drug may still be doing something long after you stop taking it.
If CTX drops more than P1NP, the ratio can look “more anabolic.”
In simple terms:
But in real life, and in drug-treated patients, this is not always true.
Here is why:
There appears to be a threshold where P1NP gets too low. When building is suppressed enough, it does not matter if breakdown is even more suppressed. There just is not enough building activity to keep improving bone over time.
This study supports that concern.
Even with long-term suppression, bone density did not keep climbing. It plateaued, then drifted.
That is not a good sign if you are trying to use this as a 15–20 year “forever plan.”
It helps. But it does not solve it.
Here is the honest take:
That is useful.
And it has one huge limitation.
This study was in women 50 to 60 who did not have osteoporosis.
This is the group that is often most likely to benefit from:
And the study excluded hormone therapy.
That matters because estradiol is FDA approved for osteoporosis prevention. And in clinical practice, properly used hormone therapy often produces strong bone results in this life stage.
So who is this drug strategy most useful for?
Probably not “the masses” in this age group.
It may be more relevant for:
If you want a clean message, here it is:
This study is a win for drug science.
It is not a replacement for a full bone plan.
In the right person, a strategy like “Reclast at baseline + year 5” may reduce fracture risk and protect bone over a decade.
But for many women in their 50s and early 60s, a smarter first-line approach is:
For most people, that plan is safer long-term and has broader health benefits.
If you are thinking about this approach, here are the questions you should ask:
If you are trying to decide whether drugs belong in your plan, the fastest way to get clarity is to learn the full framework first.
That is why we run a free Bone Health Masterclass. We cover the biggest mistakes we see and the best levers to pull first. You can also bring questions to the live Q&A.
And if you want long-term support, accountability, and community, that is what The OsteoCollective is built for.
This study suggests a single dose can suppress bone turnover for many years, and a second dose at year 5 can reduce vertebral fracture outcomes over 10 years in a prevention-level population.
No. Bone density is only one piece. Muscle, balance, protein intake, hormones, and fall risk still matter. Drugs do not replace those.
Hip bone is more cortical bone and tends to respond less to bisphosphonates than the spine.
It can be. Bone needs remodeling. Long-term suppression may raise rare risks and may limit long-term gains. This is why long-term planning matters.
Often older individuals, higher-risk patients, or people who cannot stabilize bone loss through lifestyle and hormones.
This content is for educational purposes only and is not medical advice. Do not start, stop, or change medications without speaking with your physician or qualified healthcare provider. Bisphosphonates can have serious risks and may not be appropriate for everyone, especially people with certain dental issues, kidney problems, or a history of atypical fractures.

Your Blueprint for Lasting Bone Health and Longevity
.svg)
.svg)
.svg)
.svg)
Join us LIVE July 30th, 2026 at 3:00pm EST to Learn Dr. Doug's proven framework for Osteoporosis Reversal for FREE. Yes! Reversing Osteoporosis is possible and has happened for hundreds of Dr. Doug's patients.
If you have been blind-sided, feel stuck, confused, and exhausted with your diagnosis, this Masterclass is for you!

.svg)

.svg)
